Cannabis Blood Test Duration Guide 2026: Blood, Urine, and Oral Fluid
If you search "cannabis blood test how long", the main confusion is often this: people expect one universal number, but biology and assay design make results highly conditional.
This guide answers three practical questions:
- What does blood testing actually show?
- How does it differ from oral fluid and urine windows?
- How should I act while results are being interpreted?
The core framework
For clinical and legal interpretation, test type matters more than search snippets.
- Blood: best for recent exposure assessment and timing context in specific settings.
- Oral fluid: useful for very recent use patterns but can remain positive intermittently beyond 24h in frequent users.
- Urine: usually the most sensitive for historical use and is highly influenced by cutoff level and assay choice.
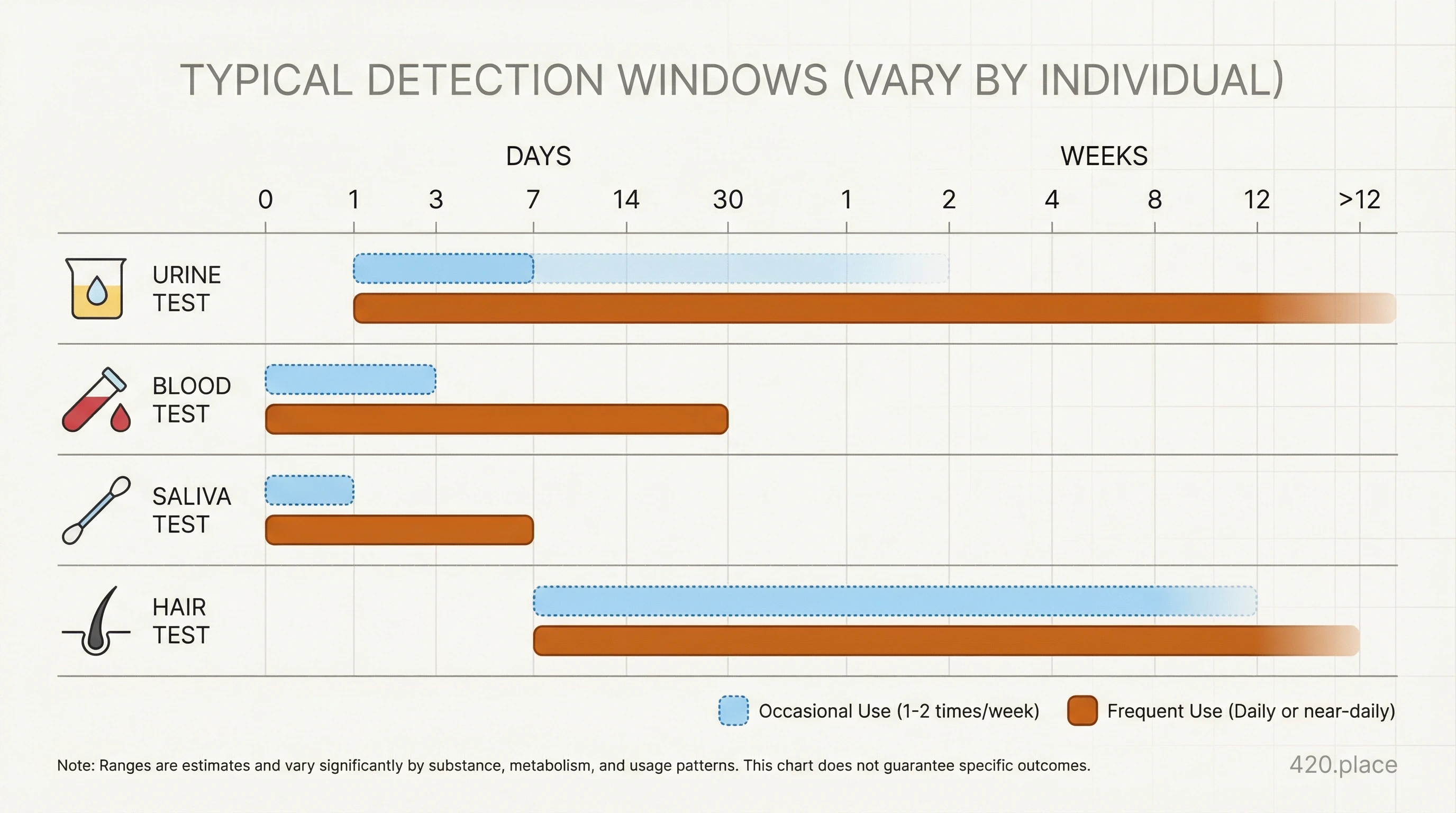
Practical duration ranges
The exact numbers shift by dose, route, frequency, and detection threshold. That said, current evidence and clinical toxicology references repeatedly show a consistent ordering:
- Blood: shortest practical window among common matrices for active THC context, with high variability in heavy or frequent use.
- Oral fluid: often short-to-medium window for recent use, but cutoffs change how long positives persist.
- Urine: shortest to very long depending on pattern, especially because the metabolite is measured after use and can persist after effects subside.
Why windows vary so much
Published toxicology analyses show that assay cutoff differences can move detection windows by days. A study comparing methods found that lower cutoffs detected cannabinoids longer than higher cutoffs, and that assay choice changed both sensitivity and timing interpretation. A high-frequency user and a single-use user should not be read through the same rule.
How to interpret blood vs urine vs oral-fluid in practice
Blood-first interpretation
Use blood findings mainly for recent exposure context, not as a simple impaired/safe score. This is especially important in workplace and safety-sensitive decisions where policy often asks for clear timelines and behavior-based review.
Oral fluid interpretation
Oral fluid is often collected when rapid, on-site decisions are needed. It is a recent-use matrix, but repeated positives over several days can occur with heavy intake, especially with sensitive cutoffs.
Urine interpretation
Urine often stays positive longer than blood/oral fluid because it tracks THC metabolites that persist after drug effects fade. Long detection windows are frequently due to cutoff and use-history factors, not sustained current intoxication.
What this means by use pattern
- Infrequent/single-use pattern: shorter windows, often back into negative sooner across matrices.
- Frequent-use pattern: widening windows and more uncertain split points, including intermittent positive/negative behavior in oral fluid monitoring.
- Chronic heavy use: longer tails are more likely in urine and sometimes in blood/fluids depending on testing design.
Action plan for high-risk decisions
Use this when result timing matters:
- Record last use time, route (smoked/vaped/edible), and time of symptom peak.
- Note sample type and cutoff level used by the lab/clinic.
- Check whether confirmatory testing was done and how chain of custody was handled.
- Compare against policy and task risk instead of relying on one number.
- If safety-sensitive work is involved, apply conservative return-to-duty checks until alertness is clearly baseline and medical guidance is clear.
Regional context: US, Canada, Germany
United States
Federal and state systems differ in how test outcomes are used in workplace and public-safety settings. The practical point is not one cutoff, but method-to-policy consistency.
Canada
Provincial policy framing is tied to licensed and medical access systems. Testing interpretation should still be read with test-method details, because a positive sample is not automatically a real-time functional label.
Germany
German frameworks for medical access and workplace safety differ from North America and are generally structured through legal medical indications and compliance logic. Use official medical context and legal channels, then apply test interpretation conservatively for safety-sensitive roles.
FAQ
Can blood testing replace my own safety judgment right after use?
No. A blood result helps place timing and exposure, but it does not automatically define functional safety in all situations.
If I am positive, how long can I still be in danger?
You may still have varying residual effects based on route, dose, and tolerance. Use symptom- and role-based safety checks, not test results alone.
Does urine always stay positive longer than blood?
Usually in regular use contexts, yes: urine can reflect exposure over a longer window than blood or oral fluid because of metabolite persistence.
Why do two people with similar use have different results?
Timing, body composition, hydration, metabolism, route, assay cutoffs, and test matrix all change outcomes.
Can I use one blog or forum result as proof of timing?
No. Prefer assay documentation, official test-protocol pages, and peer-reviewed toxicology references when making decisions.