Cannabis Testing Science 2026: How Methods, Cutoffs, and Jurisdiction Change What Results Mean
People searching cannabis testing often compare pages and get conflicting timelines. The consistent fix is to separate two levels:
- Toxicology level: matrix, assay, cutoff, and timing.
- Policy level: who uses the result and for which legal or workplace decision.
This distinction explains why two tests can both be technically correct and still lead to very different real-world outcomes.
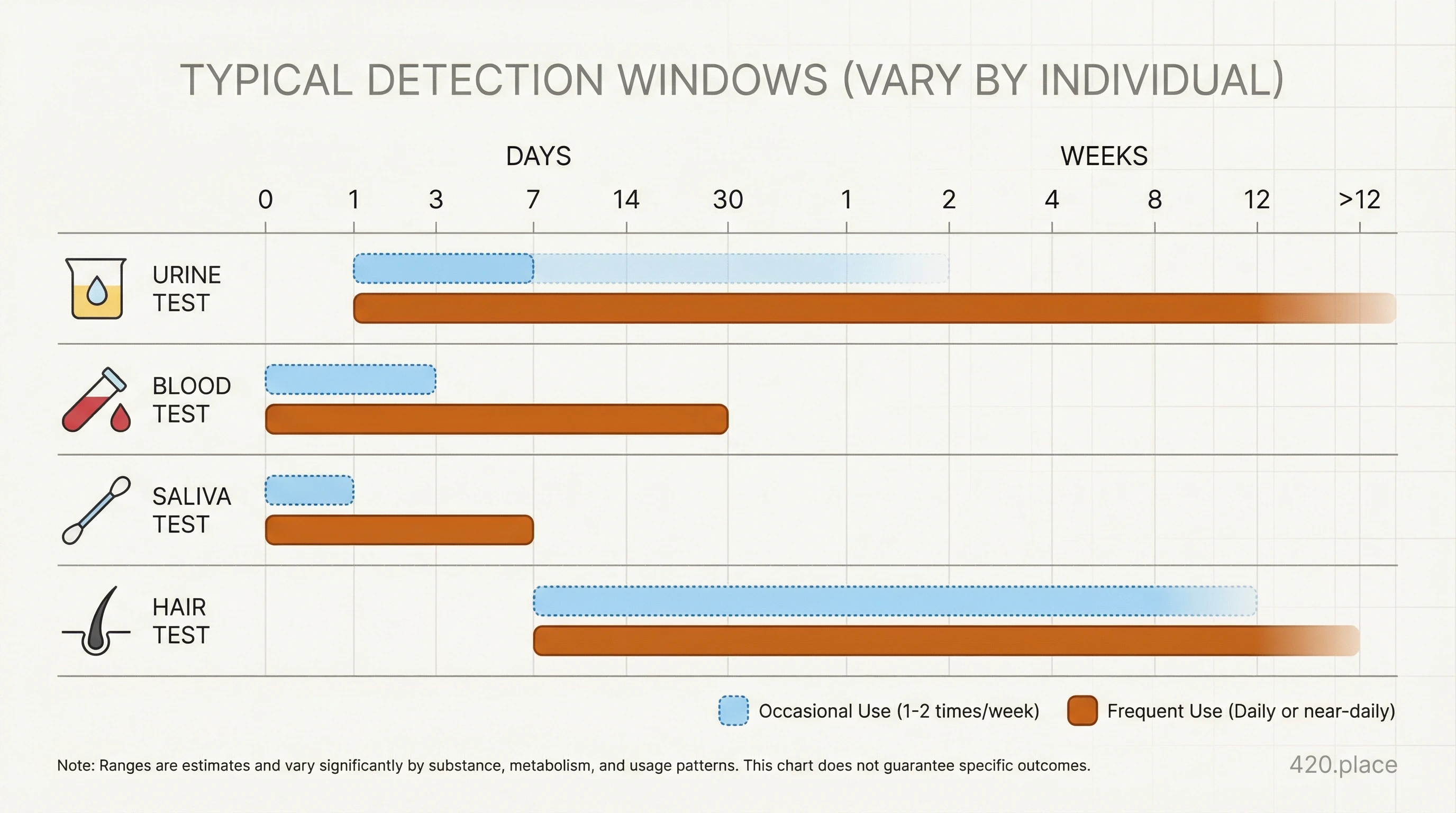
Test matrix is the first variable
Blood
Blood is mainly used for short-window and evidentiary workflows. It is often interpreted in immediate risk contexts because it reflects more recent exposure dynamics. In practice, timing still shifts with frequency of use, route, and lab protocol.
Urine
Urine commonly tracks cannabinoid metabolites and is often used for broader windows and workplace programs. It can therefore remain positive after psychoactive effects reduce.
Oral fluid (saliva)
Saliva workflows are often selected for rapid roadside or preliminary screening contexts. They are frequently useful for recent-use screening and then confirmed through additional testing depending on policy.
Hair
Hair testing is less common for immediate safety decisions. It often addresses historical exposure patterns and is interpreted within a specific compliance framework.
The practical implication is simple: compare the matrix to the question you are actually trying to answer.
Why cutoffs and methods drive timing claims
A toxicology report is never only a concentration.
- Screening methods (often immunoassays) are designed for rapid triage.
- Confirmatory methods (often GC-MS or LC-MS/MS workflows) improve specificity.
Lower cutoffs usually detect lower concentrations for longer windows. Higher cutoffs may suppress low-level positives but shorten reporting windows. This is one reason two labs can produce different headline outcomes from similar use patterns.
Because interpretation changes by lab design, you should expect variation across sites and regions even when user behavior is similar.
Where false positives and cross-reactivity usually come from
The most common risk is interpreting a screen result as final. In toxicology workflows, a single screening line is often a first-stage signal, not the final legal or clinical conclusion.
Common scientific controls include:
- Confirmatory mass-spec confirmation for suspicious or consequential positives.
- Controlled chain-of-custody and timestamping for legal cases.
- Retesting only under official protocol, especially when high-stakes decisions depend on the result.
Jurisdiction and use-case context (US, Canada, Germany)
United States
US systems are fragmented by program: workplace policies, state frameworks, and enforcement workflows can all apply different thresholds and rights processes. For the same biological pattern, a different program can reach different conclusions about next steps.
Canada
Canada's public-health and enforcement systems include oral fluid and roadside workflows, with follow-up protocols that depend on observed impairment context and case pathway.
Germany
Germany's statutory model combines defined traffic thresholds with strict evidentiary pathways. This can make test methodology and formal process more central than headline concentration interpretation alone.
How to interpret your report without overreacting
Use this 60-second workflow:
- Identify the matrix and whether it was screening or confirmatory.
- Record sampling time and last use window.
- Check cutoff or decision thresholds reported with the result.
- Compare with immediate safety context (fatigue, co-use, task risk).
- Use documented cross-region guidance only after this context is complete.
If you need to make a practical decision today--especially driving, safety-critical work, or legal response--the safest move is conservative behavior until method and legal context are clear.
Practical links and follow-up
This topic connects to three related paths in your guide stack: timing frameworks, interpretation frameworks, and enforcement context.
Related reading
- Cannabis blood test time frame
- Cannabis blood test interpretation guide
- Cannabis blood test and workplace testing guide
- Cannabis blood test police and rights guide
- How long does weed stay in your system?
FAQ
Why are results different between labs?
Different methods and cutoffs are configured for different workflow purposes. A result is only comparable when methodology and policy context are the same.
Can blood testing and urine testing be compared directly?
No. They detect different markers and are interpreted for different questions.
Is a positive screen final evidence for impairment?
Not usually. Screening is an early flag; confirmatory and clinical or legal context usually matter next.
Why are oral fluid and blood windows not the same?
They differ in biology and sampling physics. Oral fluid often supports shorter windows; blood may suit different forensic or clinical workflows.
What should I do after receiving a test result?
Document method, timing, and symptoms first, then apply the relevant protocol for your country and use case instead of acting on the number alone.